


Knee Osteoarthritis
Knee Osteoarthritis
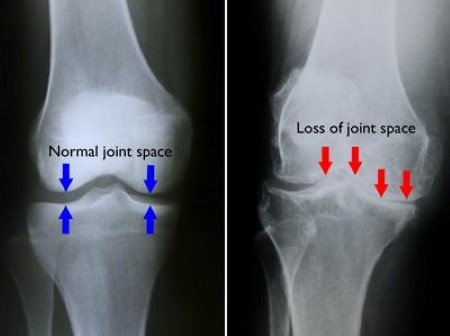
As with other joints in our body, optimal function of the knee joint requires a smooth frictionless articulating interface. This surface is provided by normal cartilage at the ends of our bones. Meanwhile, arthritis is a broad term that essentially means inflammation of a joint due to loss of cartilage and all of the subsequent associated changes. Since cartilage does not show up on X-ray, a knee joint with normal cartilage and no arthritis will appear to have a gap between the femur and tibia bones on X-ray.

Causes of Osteoarthritis
While the exact cause of arthritis is still being explored and varies from person to person, in most instances, the common initial trigger is cartilage injury. In cases of what is termed “secondary” arthritis, this cartilage damage can be related to a previous knee dislocation, injury, infection, and surgery, among other causes.
More commonly, patients present with what is termed “primary” arthritis, which is development of arthritis in the absence of the causes listed above. There are multiple theories about why some people develop primary knee arthritis. From a genetic standpoint, people with a strong family history of arthritis or a history of arthritis themselves in other joints in the body may be more likely to develop knee arthritis. In addition, development of arthritis may be associated with a history of repetitive use and loading of the knee joint over a long period of time.
Adaptations to Osteoarthritis
As the process of arthritis progresses, continued loss of cartilage will lead to narrowing and eventual complete loss of joint space as seen on X-ray. This is sometimes referred to as “bone-on-bone” arthritis. With continued cartilage degradation, there is no longer a smooth frictionless surface with knee motion and activity. As you can imagine, as joint surfaces become fissured and roughened due to arthritis (like grinding two pieces of sandpaper against one another), continuing knee activity and motion leads to inflammation of the joint.
This inflammation is the cause of pain associated with knee arthritis. The body has a remarkable way of adapting to disease processes, and in the case of knee arthritis, the body attempts to limit knee motion in several ways. First, the soft tissue capsule around the knee becomes thickened and contracted to stiffen the joint. Second, bone spurs, also referred to as osteophytes, form around the joint to further reduce motion.
Symptoms of Knee Osteoarthritis
Patients with knee arthritis most commonly experience pain and stiffness in the joint. The location of pain can vary from patient to patient, but most people report feeling a deep-seated pain all throughout the joint. Often, the pain and arthritis can start in only one compartment of the knee. This most commonly occurs in the medial (inner) aspect of the knee, yet over time it may progress to involve the lateral (outer) or patellofemoral (knee cap aspect) compartments.
Initially the pain occurs primarily with high-demand activities and certain knee positions, but as the disease progresses, pain can occur with more and more activities of daily living. With moderate to severe knee arthritis, pain then frequently occurs at night that can interfere with sleep. In fact, night-time pain and poor sleep is the most common reason why patients seek consultations with our office.
Non-Surgical Treatment
As with other chronic knee conditions, we typically recommend beginning with non-operative treatment. The primary objective is to reduce inflammation, which can be accomplished through activity modification, oral anti-inflammatory medications (NSAIDs, i.e. ibuprofen, naproxen, meloxicam, etc.), oral corticosteroids, corticosteroid (cortisone) injections, and biologic injections such as platelet-rich plasma (PRP).
Physical therapy is helpful in correcting any negative functional or postural adaptations you have made due to knee pain. Therapy will also help to strengthen the muscles surrounding the knee which will help to offload the painful cartilage adaptations in the joint.
Last, perhaps the most powerful intervention for reducing the pain associated with knee arthritis is weight loss. The reason for this is simple physics. For every 1 lb. of weight we carry, each knee experiences 5 lbs. of pressure (10 lbs. of pressure combined). So, for example, if one is able to lose 5 lbs. of weight, each knee will experience a relief of 25 lbs. of pressure (50 lbs. of pressure total)! Often patients ask ‘what is the best way to lose weight?’. While exercise can be helpful for weight loss (and is certainly beneficial for long-term health and vitality), it is often difficult for patients with knee osteoarthritis to perform regular means of exercise due to their knee pain. Fortunately, the general consensus among trained nutritionists is that about 80-85% of weight loss is achieved through dietary interventions (as opposed to exercise measures). Therefore, even patients with an inability to exercise (via walking, biking, etc.) due to their knee arthritis still have excellent odds in their favor for achieving weight loss through dietary changes. If you’d like to learn more about appropriate dietary changes you can make, we recommend consulting with a licensed nutritionist.
We offer the above medication, injection, and physical therapy measures at Kennedy-White Orthopaedic Center, and every patient’s response to the various options may be different. While none of these treatments actually reverse the progression of arthritis, they can provide pain and symptom relief for long periods of time.
Surgical Treatment
If non-operative treatment methods have failed to provide lasting symptom relief, then surgical treatment may be offered. Due to the nature of the disease process, minimally-invasive arthroscopic procedures for knee osteoarthritis are generally avoided due to their lack of lasting relief. The exception to this is in the case of an entrapped loose body (from a degenerative meniscus tear or cartilage flap) which has become lodged in the joint and limits knee motion all-together. In these rarer instances, an arthroscopic procedure to remove the loose body to restore range of motion may be appropriate. We would be happy to discuss if this is an option for you during your consultation.
Ultimately, the definitive treatment for end-stage knee arthritis is knee arthroplasty (replacement). This involves replacing the arthritic femur and tibia bones with metal implants with a highly cross-linked polyethylene plastic liner between them to allow for motion of the new joint. Dr. Koscso performs this procedure through an advanced, robotic-assisted technique with precise bone cuts to optimize outcomes of the operation. Based on the extent of osteoarthritis in the knee, one of the below procedures may be undertaken:
Unicompartmental Knee Arthroplasty (partial knee replacement). If the arthritis is limited to only one compartment of the knee joint (for example, the medial compartment), then a partial knee replacement may be an option. This procedure would obviously involve only replacing the diseased compartment with metal and a polyethylene liner. The benefit to this procedure is that it preserves the remainder of the native, healthy knee joint. It also tends to lead to less pain and a quicker recovery post-operatively with a higher level of activities that patients can expect to return to.



Total Knee Arthroplasty (replacement). Once a patient’s arthritis involves multiple compartments of the knee, a total knee replacement is often the appropriate operation performed. This involves removing the arthritic portions of the femur and tibia bones through precise bony cuts made with robotic-assistance. New metal implants and a highly cross-linked polyethylene liner create the new knee joint. This operation is highly successful at relieving the pain associated with arthritis and allowing patients to return to a higher level of activity postoperatively.



Post-Operative Recovery
For a comprehensive reading of the expected post-operative recovery, including restrictions, physical therapy progressions, and return to work/sport guidelines after partial or total knee replacement surgery, please see our corresponding protocol on our physical therapy protocols page.

About the Author

Dr. Jonathan Koscso is an orthopedic surgeon and sports medicine specialist at Kennedy-White Orthopaedic Center in Sarasota, FL. Dr. Koscso treats a vast spectrum of sports conditions, including shoulder, elbow, knee, and ankle disorders. Dr. Koscso was educated at the University of South Florida and the USF Morsani College of Medicine, followed by orthopedic surgery residency at Washington University in St. Louis/Barnes-Jewish Hospital and sports medicine & shoulder surgery fellowship at the Hospital for Special Surgery in New York City, the consistent #1 orthopaedic hospital as ranked by U.S. News & World Report. He has been a team physician for the New York Mets, Iona College Athletics, and NYC’s PSAL.
Disclaimer: All materials presented on this website are the opinions of Dr. Jonathan Koscso and any guest writers, and should not be construed as medical advice. Each patient’s specific condition is different, and a comprehensive medical assessment requires a full medical history, physical exam, and review of diagnostic imaging. If you would like to seek the opinion of Dr. Jonathan Koscso for your specific case, we recommend contacting our office to make an appointment.