

PCL Injury
Posterior Cruciate Ligament (PCL) Injury
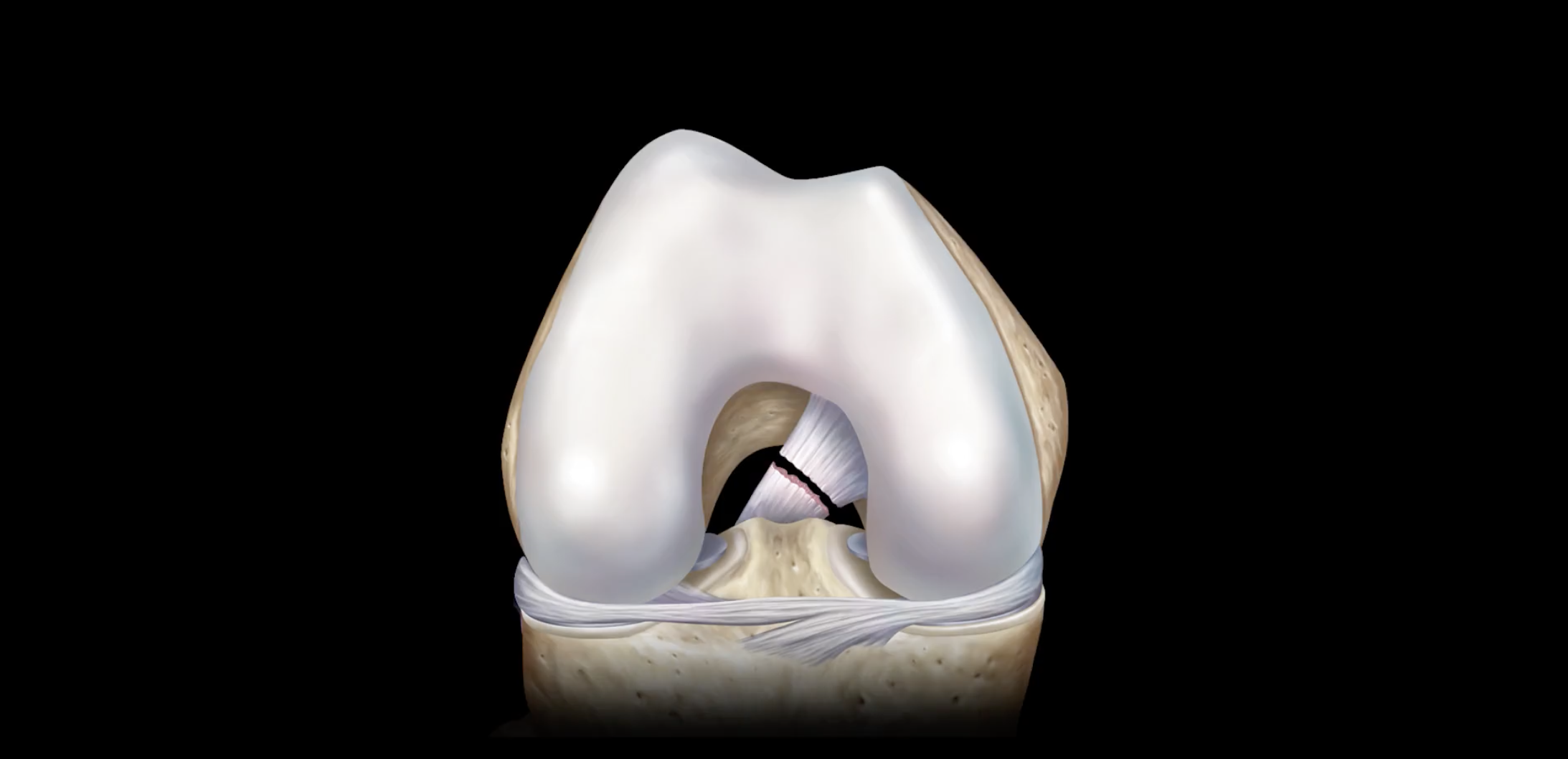
The posterior cruciate ligament (PCL) is attached to the front of the femur (thigh bone) and travels through the center of the knee behind (posterior) the anterior cruciate ligament (ACL) to the back of the tibia (shin bone). These ligaments form an “X” and, together, play an important function in limiting forward and backward movement of the tibia. The PCL is formed from two parts that combine into the strongest of the four main knee ligaments approximately the size of one’s little finger. Due to its strength, the PCL is not injured as often as the other knee ligaments; although, a substantial force to the anterior knee and shin can damage this ligament. Athletes involved in contact sports are more likely to experience a PCL injury. However, a motor vehicle collision or falling directly onto a bent knee can also produce a tear within the posterior cruciate ligament.
Orthopedic Surgeon and Sports Medicine specialist, Dr. Jonathan Koscso, successfully diagnoses and treats patients in Sarasota, FL and the surrounding Gulf Coast region who have experienced a knee PCL injury.
For a comprehensive overview of the relevant anatomy, biomechanics, diagnostic tools, and treatment algorithm for PCL injuries, the below video is helpful.

Types of PCL Injuries
PCL injuries, similar to other ligament injuries, are graded on the severity of damage sustained by the posterior cruciate ligament and assigned one of three classifications.
Grade 1: Minimal damage to the ligament from being pulled or stretched; the joint remains stable.
Grade 2: The ligament partially detaches from being stretched. This injury results in a partial tear, or PCL sprain, and the knee joint remains generally stable.
Grade 3: The ligament is torn into two separate pieces, also known as a rupture. The knee is no longer stable with a complete PCL tear.

Symptoms of a PCL Injury
Damage to the posterior cruciate ligament is often a secondary injury as a result of significant trauma to the knee; it is rare that only the PCL is damaged after a traumatic event. It is important to consult an orthopedic knee specialist if a PCL injury is suspected. Common complaints of a PCL injury include:
Pain along the outside of the knee, especially when increasing speed on a run
Difficulty walking downstairs or slowing down on a run
Swelling
Difficulty with pivoting or twisting the affected lower leg
To diagnose a PCL injury, Dr. Koscso will perform a comprehensive medical history and thorough physical examination to evaluate knee stability through a number of tests involving the affected lower leg. Diagnostic imaging, such as x-rays and magnetic resonance imaging (MRI), may be needed to determine the extent of a PCL injury as well as identify any damage to the other structures within the knee complex.
Non-Surgical Treatment of a PCL Injury
Conservative therapy may be sufficient to resolve a posterior cruciate ligament injury if no other structures within the knee complex were also injured. Rest, ice, compression, and elevation (RICE), as well as a specialized brace to provide stability and avoiding weight-bearing can aid in proper healing of the ligament. Non-steroidal anti-inflammatory medications (ibuprofen, naproxen, meloxicam, etc.) can be taken as directed to diminish the pain and swelling associated with this condition. Once Dr. Koscso determines it’s safe, a physical rehabilitation program to restore range of motion and strength to the knee will be prescribed.
Surgical Treatment of a PCL Injury
When other ligaments or structures of the knee complex are involved in a PCL injury, or in the event conservative therapy is unsuccessful, surgical intervention may be needed to restabilize the knee joint. A torn PCL is surgically reconstructed using a tendon graft, either from the patient (autograft) or donor tissue (allograft). A tunnel is drilled into the femoral and tibial attachments of the native PCL and a graft is passed through the tunnels and secured using surgical screws or anchors. This operation is typically performed along with reconstruction of other damaged ligaments in the knee, and so the extent of surgery can vary from patient to patient.

Graphic representation of a full-thickness PCL injury (left) that has been reconstructed using a tendon graft (right) with tunnels that have been drilled through the femur and tibia.
Post-Operative Recovery
For a comprehensive reading of the expected post-operative recovery, including restrictions, physical therapy progressions, and return to work/sport guidelines after PCL repair/reconstruction surgery, please see our corresponding protocol on our physical therapy protocols page.
About the Author

Dr. Jonathan Koscso is an orthopedic surgeon and sports medicine specialist at Kennedy-White Orthopaedic Center in Sarasota, FL. Dr. Koscso treats a vast spectrum of sports conditions, including shoulder, elbow, knee, and ankle disorders. Dr. Koscso was educated at the University of South Florida and the USF Morsani College of Medicine, followed by orthopedic surgery residency at Washington University in St. Louis/Barnes-Jewish Hospital and sports medicine & shoulder surgery fellowship at the Hospital for Special Surgery in New York City, the consistent #1 orthopaedic hospital as ranked by U.S. News & World Report. He has been a team physician for the New York Mets, Iona College Athletics, and NYC’s PSAL.
Disclaimer: All materials presented on this website are the opinions of Dr. Jonathan Koscso and any guest writers, and should not be construed as medical advice. Each patient’s specific condition is different, and a comprehensive medical assessment requires a full medical history, physical exam, and review of diagnostic imaging. If you would like to seek the opinion of Dr. Jonathan Koscso for your specific case, we recommend contacting our office to make an appointment.