

Meniscus Tear
Meniscus Tear
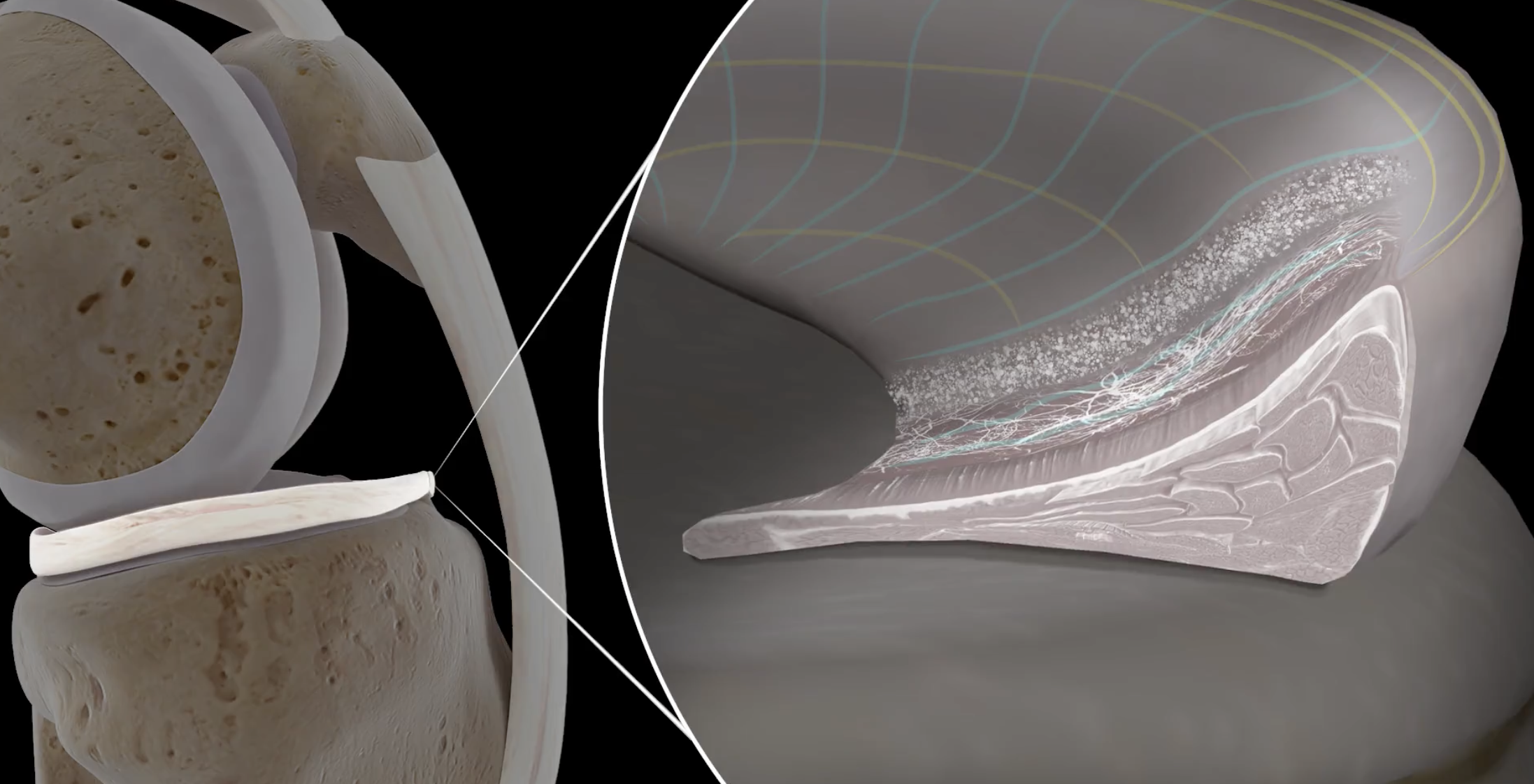
Located between the femur (thigh bone) and tibia (shin bone) are two “C” shaped shock-absorbing cartilage structures known as the menisci (singular = meniscus). The menisci are made up of the medial (inner) meniscus and the lateral (outer) meniscus. The medial meniscus, along the inner portion of the knee, bears up to 50% of the stress load exerted on the medial compartment of the knee. The lateral meniscus, along the outer portion of the knee, bears up to 80% of the stress load exerted on the lateral compartment of the knee. The menisci function as a shock absorber between the femur and tibia and also provides lubrication for the knee joint to move easily. An additional role of the menisci is protecting the ligaments from outside forces and providing stability to the knee joint. A tear within a meniscus can be caused by forceful knee rotation with the full weight of the body on the knee. This type of injury is one of the most common injuries seen in athletes, but individuals can experience a meniscus tear even with routine activities of daily living.
The bones and cartilage of the knee can experience added stress and degeneration in the absence of a complete and healthy meniscal fibrocartilage ring. Meniscal deficiency (and eventual osteoarthritis) occurs when the knee joint breaks down without the presence of a healthy meniscus. This can occur from a degenerative condition, a hereditary condition, or from a misshapen meniscus. Additionally, meniscal tears are often associated with other knee-related injuries such as ACL tears, and treatment of all associated conditions is crucial in restoring the knee to an optimally functioning state.
Orthopedic Surgeon and Sports Medicine specialist, Dr. Jonathan Koscso, successfully diagnoses and treats patients in Sarasota, FL and the surrounding Gulf Coast region who have experienced a meniscus injury.

Symptoms of a Meniscus Tear
There are generally two broad categories in considering the cause of meniscal tears: acute and chronic, or degenerative. Acute meniscus tears are generally associated with single, discreet injuries and tend to occur in younger patients (i.e. a football player being tackled and tearing their ACL and a meniscus, or a tennis player pivoting during a backhand and experiencing sharp, sudden pain in their knee). These tears, compared to their chronic, or degenerative, counterparts tend to have a higher likelihood of being repaired with a minimally-invasive arthroscopic surgery (see below). Chronic meniscus tears, on the other hand, are generally associated with a longstanding achy pain in a part of the knee that tends to flare up after bouts of heavy activity. These tears are unfortunately frequently associated with arthritis- the longstanding breakdown of the articular cartilage in the knee. Additional symptoms of chronic meniscus tears include:
Swelling and stiffness
“Locking” or “catching” of the knee
A “pop” can sometimes be heard with a given injury
Decreased knee range of motion
Knee instability or “buckling” episodes
To diagnose a meniscal tear, a comprehensive medical history, including how the injury occurred, will be performed by Dr. Koscso. A physical examination will be performed involving an evaluation for areas of pain and tenderness and range of motion will be assessed. Diagnostic imaging, such as x-rays and magnetic resonance imaging (MRI), may be requested to determine the extent of the injury and confirm a meniscus tear diagnosis. MRI is often additionally helpful in identifying any other associated injuries to the knee.


Non-Surgical Treatment
If a meniscus tear is small and the patient does not experience instability as a result of the injury, conservative therapies may be appropriate to heal the tear. A combination of rest, ice, and non-steroidal anti-inflammatory medications can be used for pain management and reduce inflammation. When deemed appropriate, Dr. Koscso will recommend a physical rehabilitation program to restore range of motion and strength to the knee.
Additionally, the chronic degenerative meniscal tears described above can often be managed non-surgically with these conservative measures. A key management strategy for these tears is recognizing the activity loads that tend to flare up the tear and lead to pain, and then to avoid those activities as much as able, or to at least be prepared with ice and an anti-inflammatory medication later in the day. The caveat to this non-surgical approach, however, is that if a tear causes acute “locking” of the knee (it becomes difficult to fully bend or straighten the knee due to the tear), then a surgical approach may be appropriate.
Surgical Treatment
If conservative therapy is unsuccessful, or if an acute tear occurs in an otherwise perfectly healthy knee, Dr. Koscso may recommend an arthroscopic meniscus repair or meniscectomy. This minimally invasive procedure involves a small camera (arthroscope) and specialized surgical instruments to complete the necessary surgery. Based on the intraoperative findings, Dr. Koscso may implement one or more of the following surgical techniques:
Meniscal Repair: This procedure is ideal for tears that occur within the outer third of the meniscus with a healthy blood supply. The torn portions of the meniscus are reattached using special surgical sutures that are secured within the knee.
Biologic Augmentation: This technique utilizes the patient’s own bone marrow, known as Bone Marrow Aspirate Concentrate (BMAC), or platelet-rich plasma (PRP) to stimulate healing at the meniscus repair site. Biologic Augmentation is often performed in conjunction with a meniscal repair.
Meniscectomy: This technique is reserved for patients with larger, complex tears that are not amenable to being repaired with sutures. Chronic, degenerative tears often fall into this category and unfortunately cannot be repaired. During this procedure, Dr. Koscso removes the portions of the meniscus that are non-repairable while leaving all healthy portions of the meniscus to preserve as much native tissue as possible.
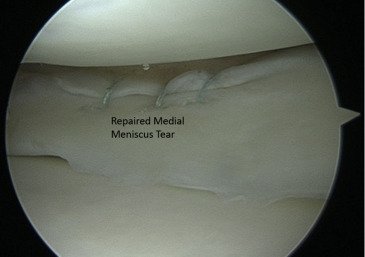
Arthroscopic image of a right knee medial meniscus tear that has been repaired with three sutures.

Arthroscopic image of a left knee medial meniscus oblique tear in the relatively avascular (inner) portion of the meniscal tissue. Due to the poor healing potential in this portion of the meniscus, a repair was unable to be carried out. Accordingly, the torn portion of the meniscus was excised and smoothed with an arthroscopic instrument. Though not restoring the full, native function of an intact meniscus, this procedure is often successful at relieving the pain associated with a tear.
Post-Operative Recovery
For a comprehensive reading of the expected post-operative recovery, including restrictions, physical therapy progressions, and return to work/sport guidelines after meniscus surgery, please see our corresponding protocol on our physical therapy protocols page.
About the Author

Dr. Jonathan Koscso is an orthopedic surgeon and sports medicine specialist at Kennedy-White Orthopaedic Center in Sarasota, FL. Dr. Koscso treats a vast spectrum of sports conditions, including shoulder, elbow, knee, and ankle disorders. Dr. Koscso was educated at the University of South Florida and the USF Morsani College of Medicine, followed by orthopedic surgery residency at Washington University in St. Louis/Barnes-Jewish Hospital and sports medicine & shoulder surgery fellowship at the Hospital for Special Surgery in New York City, the consistent #1 orthopaedic hospital as ranked by U.S. News & World Report. He has been a team physician for the New York Mets, Iona College Athletics, and NYC’s PSAL.
Disclaimer: All materials presented on this website are the opinions of Dr. Jonathan Koscso and any guest writers, and should not be construed as medical advice. Each patient’s specific condition is different, and a comprehensive medical assessment requires a full medical history, physical exam, and review of diagnostic imaging. If you would like to seek the opinion of Dr. Jonathan Koscso for your specific case, we recommend contacting our office to make an appointment.