


Patellar Instability
Patellar Instability
The patella (knee cap) is an important bone in the front of the knee that aids in connecting the muscles of the thigh to the lower leg and, therefore, assists in straightening one’s knee from a flexed position. This fundamental motion is necessary for walking, running, jumping, or any physical activity we do on our feet. The patella is held in its anatomic place by several key structures including ligaments, muscles, and bony grooves at the end of the femur (thigh bone). Sometimes, the patella can dislocate from this usual anatomic position from an injury which can be quite painful and lead to difficulty with performing ongoing sporting activities.
Patellar instability is a condition associated with dislocations and/or repeated subluxations (abnormal shifting) of the patella that cause pain and limit one’s ability to remain active. This condition can arise in athletes of all ages, though it is typically seen in younger patients with a number of various risk factors such as malalignment of the bones around the knee, muscle imbalances around the knee and hip, or looser soft tissues and ligaments around the knee. In patients with patellar instability, the goal is to address and correct these risk factors through the least-invasive means possible to a point that allows the patient to return to the activities they love doing.
Orthopedic Surgeon and Sports Medicine specialist, Dr. Jonathan Koscso, successfully diagnoses and treats patients in Sarasota, FL and the surrounding Gulf Coast region who have experienced patellar instability.

Symptoms of Patellar Instability
Patients who experience patellar instability will typically experience an initial, specific injury to their knee during a sporting event in which they were attempting to twist or pivot and had sudden, sharp pain in the knee. Other symptoms associated with this injury include:
knee swelling, or effusion.
difficulty with weight bearing.
Pain along the joint spaces of the knee, or especially along the medial (inner) aspect of the knee.
Apprehension, or a sense of anxiety, when the patella is manually moved towards the outer side of the knee.
Often times, patients can experience more than 1 episode of a patellar dislocation or subluxation, with the ongoing inability to perform in their sport. In these instances, a careful assessment and discussion of proper treatment becomes essential.
To diagnose patellar instability, Dr. Koscso will perform a comprehensive medical history and inquire about the events leading up to the injury and/or repeated dislocations and subluxations. He will also perform a thorough physical examination including an evaluation for areas of pain and assessing knee range of motion and stability. Diagnostic imaging such as x-rays and magnetic resonance imaging (MRI) may be requested to confirm a diagnosis of patellar instability and identify any damage to other structures within the knee joint. For example, patients with patellar instability have nearly always injured a vital ligament on the medial (inner) part of the knee called the Medial Patellofemoral Ligament (MPFL) which stabilizes the patella in its anatomic location. In more substantial injuries, however, patients can also damage the articular cartilage along the patella and underlying femoral bone.
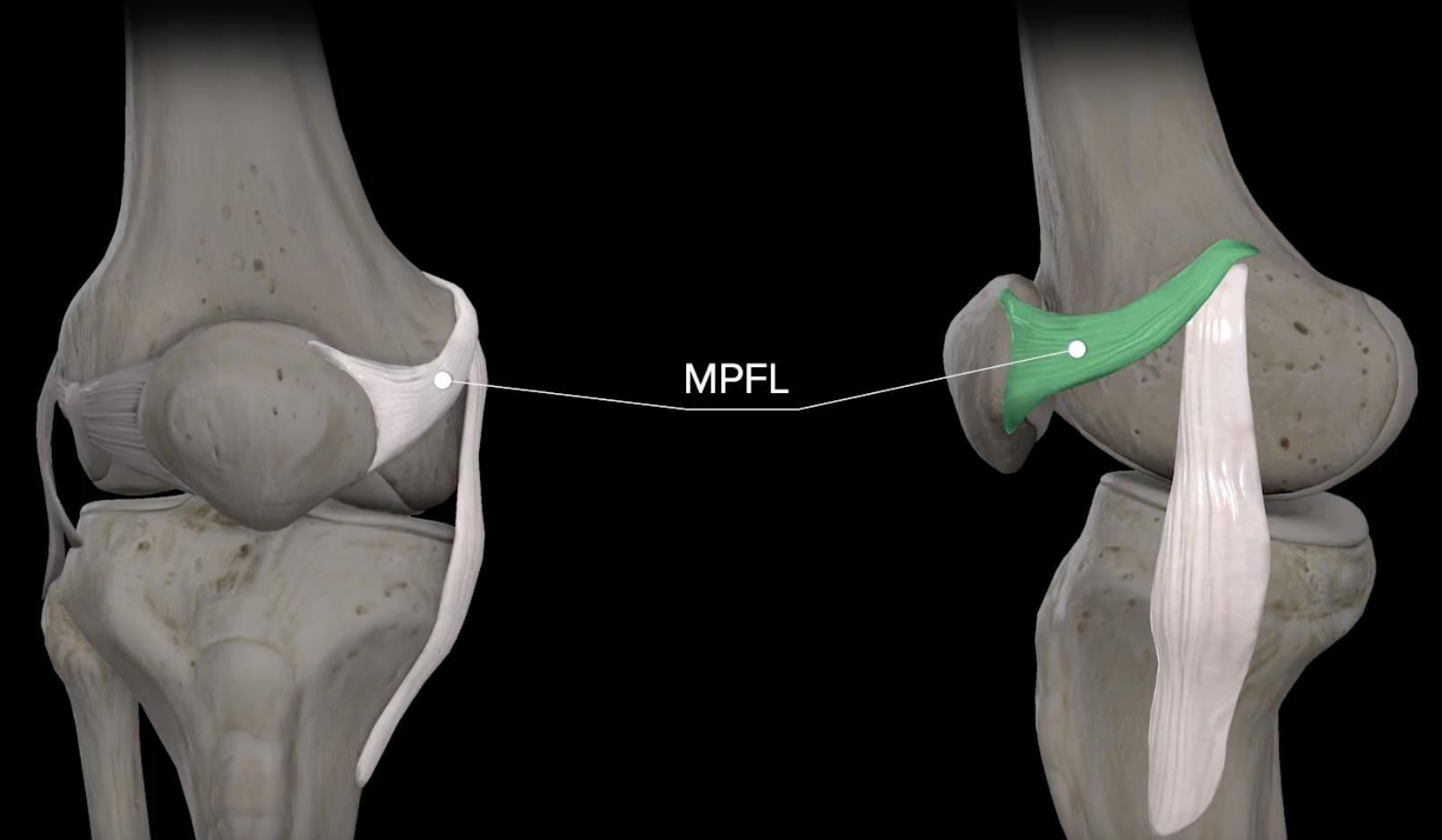

(Left) The MPFL is an important ligament on the medial (inner) aspect of the knee which functions to help stabilize the patella within its bony groove on the femur bone. (Right) this axial MRI image of a left knee after an acute patella dislocation shows injury to the MPFL as well as multiple osteochondral (combination of cartilage and underlying bone) fractures on the medial patella and underlying femur bone.
Non-Surgical Treatment
After an acute patellar dislocation, the initial goal is to reduce pain and swelling in the knee through conservative measures. Rest, ice, compression, and elevation (RICE) of the knee is important to allow the patient to mobilize without significant pain. Tylenol/acetaminophen and non-steroidal anti-inflammatory drugs such as ibuprofen, naproxen, meloxicam, etc. are also helpful to reduce pain and inflammation. Once pain has been minimized, a regimen of physical therapy is important to regain normal knee range of motion and strength. Building on this, ongoing physical therapy aims to address various muscle imbalances and coordination deficits that likely contributed to the initial injury.
For some patients who have experienced a single patellar dislocation event, the above measures coupled with an ongoing dedicated knee strengthening and conditioning program may be all that is needed to adequately treat their patellar instability. Unfortunately, however, there are a number of risk factors for recurrent patellar instability that are highly variable from patient to patient and should be assessed by an experienced Sports Medicine surgeon to determine the risk of re-injury with conservative treatment alone.
Surgical Treatment
In patients with patellar instability with associated damage to other knee structures such as the articular cartilage or even bony fractures, surgery may be an appropriate first-line treatment once the swelling has been treated and knee range of motion restored. Likewise, some younger and more active patients may benefit from a surgical discussion after a single dislocation event without other associated knee damage, especially if they have risk factors for recurrent instability. Last, patients who are experiencing recurrent dislocations/subluxations of the patella that is limiting their activity would likely benefit from a surgery.
Should a surgical plan be decided upon by the patient and Dr. Koscso, the specific treatment strategy can vary widely from patient to patient. Typically, the patient will undergo a knee arthroscopy- a minimally invasive procedure to look inside the knee with a small arthroscope (camera) to assess any damage to the articular cartilage, menisci, or ligaments inside the knee. Following this, a number of additional procedures may be performed to correct the instability and minimize the risk for future dislocations. These include:
Medial Patellofemoral Ligament (MPFL) repair or reconstruction. As stated above, the MPFL is a vital ligament on the inner aspect of the knee that stabilizes the patella in its anatomic position. It is nearly always injured with a patellar dislocation and warrants repair (in select cases) or reconstruction with a tendon graft either from another part of the patient’s body or from a cadaver.
Tibial tubercle osteotomy. Patients with patellar instability often have bony malalignment around their knee which can predispose the patella to subluxating or dislocating laterally (towards the outer side of the knee). In these cases, a procedure to cut the tibia (shin bone) and change its alignment can reduce the risk of future instability.
Trochleoplasty. Some patients with patellar instability have bony malalignment of the groove (trochlea) at the end of the femur which the patella normally “sits” in. This condition is known as “trochlear dysplasia”. In select patients with severe trochlear dysplasia, a procedure to correct the bony geometry of this groove to a more normal shape can be performed.
Distal femur osteotomy. In rare cases, patients with patellar instability may have an abnormally rotated femur (thigh bone) to an extent that it allows the patella to slide out of its normal position under much lower physical loads. In these cases, a procedure to cut the femur bone and correct its rotation may be appropriate.

MPFL injury (left) before MPFL reconstruction with a tendon graft (right) to restore the stabilizing function of the ligament.


Tibial tubercle osteotomy graphic representation (left) showing that the tibial tubercle has been cut and shifted medially to reduce the risk of future patellar instability. AP and lateral x-rays (right) of a right knee after this procedure.
Post-Operative Recovery
For a comprehensive reading of the expected post-operative recovery, including restrictions, physical therapy progressions, and return to work/sport guidelines after patellar instability surgery, please see our corresponding protocol on our physical therapy protocols page. Note that the specific PT protocol after surgery is dependent on which of the above procedures are performed.
About the Author

Dr. Jonathan Koscso is an orthopedic surgeon and sports medicine specialist at Kennedy-White Orthopaedic Center in Sarasota, FL. Dr. Koscso treats a vast spectrum of sports conditions, including shoulder, elbow, knee, and ankle disorders. Dr. Koscso was educated at the University of South Florida and the USF Morsani College of Medicine, followed by orthopedic surgery residency at Washington University in St. Louis/Barnes-Jewish Hospital and sports medicine & shoulder surgery fellowship at the Hospital for Special Surgery in New York City, the consistent #1 orthopaedic hospital as ranked by U.S. News & World Report. He has been a team physician for the New York Mets, Iona College Athletics, and NYC’s PSAL.
Disclaimer: All materials presented on this website are the opinions of Dr. Jonathan Koscso and any guest writers, and should not be construed as medical advice. Each patient’s specific condition is different, and a comprehensive medical assessment requires a full medical history, physical exam, and review of diagnostic imaging. If you would like to seek the opinion of Dr. Jonathan Koscso for your specific case, we recommend contacting our office to make an appointment.